
The "No" That Isn’t Final: Why Prescriptions Are Denied
- Mar 16
- 6 min read
Imagine you are in the final round of a game show. One last question stands between you and a life‑changing prize. The host reads the question, the clock starts ticking, and instead of thinking, you freeze. You assume you cannot possibly get it right, so you put the buzzer down and walk away.
That is exactly how the denial system is designed to work. When you get an “adverse determination” letter about your prescription, you are meant to feel overwhelmed and defeated before you even read the second paragraph. Yet buried in that dense letter is the answer key: the specific reason they said no and the clues to what would make them say yes.
Here is the industry’s open secret. In Medicare Advantage plans, more than eight in ten prior authorization denials that are appealed, about 80.7 percent, are fully or partially overturned, according to a 2024 analysis by Kaiser Family Foundation. But only a small share of denials are ever appealed at all, and the system quietly depends on you never questioning that first no.
The Open Secret: Why They Count on You Not Reading the Fine Print
PBMs and insurers know most people will not read a three‑page denial letter with a fine‑tooth comb. They count on you skimming the words “not medically necessary” or “not covered,” feeling discouraged, and giving up.
In reality, that letter is more like a puzzle than a verdict. Each phrase “prior authorization required,” “step therapy,” “quantity limit,” “not on formulary” points to a specific rule they say you did not meet. Once you understand which bucket your denial falls into, you can decide what needs to change: information, coding, or sometimes the plan’s own interpretation of your case.
Meanwhile, denial rates keep climbing. An analysis of more than 4 billion private‑insurance claims found that prescription drug denial rates rose from 18.3 percent in 2016 to 22.9 percent in 2023, a 25 percent jump, showing just how often these “no’s” now appear in people’s lives. Yet despite that rise, most patients never push back.
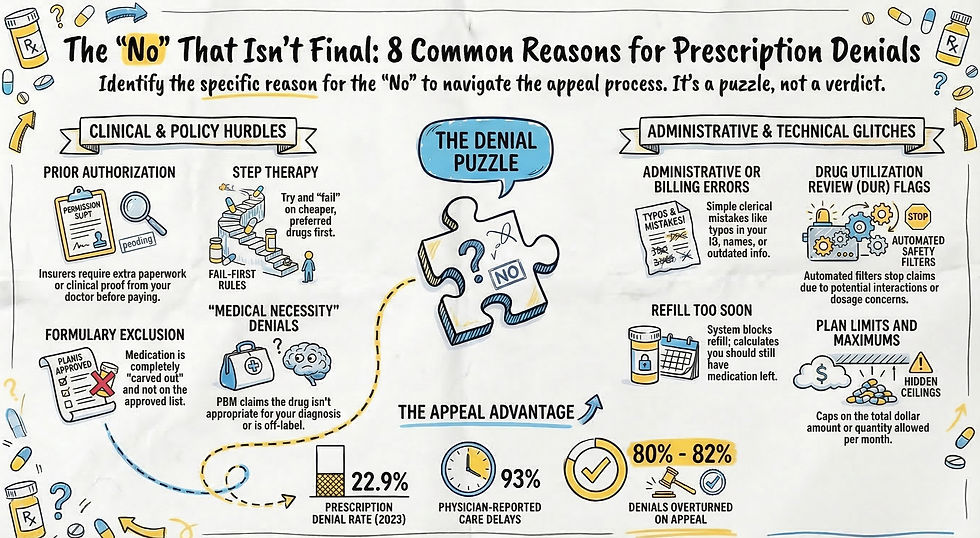
The 8 Most Common Reasons Prescriptions Are Denied
When a PBM says no, it usually fits into one of eight categories. Knowing which one you are dealing with is the first step toward understanding your letter instead of fearing it.
Prior Authorization Required
Translation: “We want more paperwork before we pay.” The plan is asking your doctor to send in extra information (e.g. office notes, lab results, or treatment history) before the medication will be covered. If that information is never sent, or if key details are missing, the request is denied.
Pro Tip: If you have been on a medication that now requires prior authorization or is ready to be re-authorized, be sure your insurer reviews your case under "Re-authorization Criteria" or "Continuation of Therapy" benchmarks. This information should be in their Clinical Criteria policy for your specific condition/medication. These standards are often significantly easier to meet than initial authorization rules because they prioritize stability over experimentation.
Formulary Exclusion
Every plan keeps a list of drugs it is willing to cover called a formulary. When your medication is “excluded,” it means the plan has chosen not to cover it at all. In simple terms, “carved out completely” means the drug is not on the list in any form—no brand, no generic, no special exception, so the default answer is “we do not pay for this medication under this plan.”
Step Therapy (“Fail‑First” Rules)
Step therapy means the plan wants you to “fail” cheaper options before it will cover the medication your doctor picked first. The denial letter might say you must try “preferred” drugs, even if you have already tried them in the past or your doctor knows they will not work for you.
“Medical Necessity” Denials
Here, the PBM claims your medication is “not medically necessary” for your diagnosis or that it is being used in a way they do not approve, such as off‑label use, even when your doctor is following accepted medical guidelines. The decision is usually based on internal criteria most patients and even many doctors never see.
Drug Utilization Review (DUR) Flags
DUR is the plan’s safety filter. Sometimes these flags protect patients, but other times they are rigid rules that do not match your real‑world situation. Your claim can be stopped if the system flags:
A possible interaction with another drug
A dose outside their preferred range
A quantity that looks too high or too frequent
Administrative or Billing Errors
Many “no’s” have nothing to do with your health at all. The letter may sound clinical, but the root problem can be as simple as a mis‑keyed digit. Common culprits include:
Misspelled name or wrong date of birth
Old insurance card on file
Typo in your member ID or group number
Pharmacy billing the wrong plan or using the wrong drug code
Refill Too Soon
The system calculates how long your last prescription should have lasted and blocks any refill before that date. If your dose changed, you lost medication, or your schedule shifted, the computer will still mark it as “too soon” until someone updates the record.
Plan Limits and Maximums
Some plans set hidden ceilings: a maximum total dollar amount, a set number of fills, or a hard cap on how many pills or injections you can receive within a certain time frame. The denial may reference “quantity limits” or “benefit maximums,” even though those limits were never clearly explained when you enrolled.
Bureaucratic Amnesia: When They Pretend Your History Doesn’t Exist
If you have been stable on a medication for months or years, a denial can feel like someone has erased your medical story and started from page one. That is bureaucratic amnesia.
PBMs often process renewals as if you were a brand‑new patient. They ignore years of successful treatment and look only at whether you match their initial approval checklist right now. That makes it easier for them to push “non‑medical switching”—moving you off a medication that works and onto a cheaper alternative—not because your health changed, but because their cost calculations did.
From your side, it sounds like:
“We don’t see that you tried the cheaper drug,” even if you did years ago.
“You must meet initial criteria,” even though you are clearly in continuation‑of‑therapy territory.
“We need proof this drug is still necessary,” despite no problems and long‑term stability.
This is not a personal failure; it is a system wired to forget the parts of your history that cost money to honor.
Administrative Errors: The “No” That Should Never Have Happened
Some of the most stressful denials come down to nothing more than clerical mistakes and siloed systems. Each department sees a narrow slice of your file, so they pass you around like a hot potato while insisting “the computer says no.”
Common error‑based denials include:
The prescriber’s NPI or tax ID is entered incorrectly
The medication is billed under the wrong benefit (pharmacy vs. medical)
Your plan year changed and the old policy is still attached to your profile
A representative attached the wrong denial code to your case
In these situations, the denial letter may still use intimidating language, but fixing the underlying data is often all it takes to clear the roadblock. Unfortunately, many people never find that out. They just assume the denial reflects a final medical judgment and stop trying to fill the prescription. One industry analysis notes that while many replacement claims for the same drug are eventually approved after a denial, some patients give up entirely and go without needed medication out of sheer frustration.
Why Understanding “Why” Matters
When you strip away the jargon, a denial letter is telling you one key thing: “Here is the reason we said no.” That reason might be about missing paperwork, a plan rule, a coding error, or the PBM’s narrow definition of “medical necessity.”
If you do not know which category your denial falls into, it all feels like one giant, faceless rejection. Once you do know, you can decide what comes next—whether that is asking your doctor for stronger clinical support, correcting basic information, or simply insisting that your long history on a medication be recognized instead of erased.
If you want to discover how to build the clinical argument that defeats a “medical necessity” denial, see my blueprint for an LOMN, The Ultimate Clinical Argument, where I walk through how doctors can translate your story into the kind of evidence reviewers cannot ignore. And when you are ready to learn the specific “power moves” and legal codes that crack the toughest “no’s,” check out The Ongoing Battle: My Personal Fight Against the PBM Machine.



Comments