
Beyond the Rejection: Power Moves for Overcoming Denials
- Mar 16
- 7 min read
I have been navigating prescription denials for over a decade. I have spent hours on hold, filed more appeals than I can count, and learned, sometimes the hard way, exactly which moves work and which ones just keep you spinning. What follows is the complete playbook: eleven strategies that can take you from frustrated patient to the most persistent, well-documented, legally-informed problem the Pharmacy Benefit Manager (PBM) has ever had to deal with.
That last part matters. PBMs count on patients giving up. They win when you abandon treatment out of exhaustion. These strategies exist to make abandonment impossible, and to make approving your claim the path of least resistance for the insurer.
A note before we begin: several strategies below reference Tennessee state law. If you live outside Tennessee, the principles are the same — the specific code numbers will differ. Check your state's Department of Insurance website or use this link to state PBM policies to find your state's PBM laws and protections.

1. Maintain a Meticulous Paper Trail
In the insurance world, a verbal promise carries zero weight unless you document it. Every single interaction (calls, portal messages, faxes, texts) needs to be logged with four data points: the exact date and time, the name and employee ID of every representative you speak with, the ticket or reference number generated by the call (never hang up without one), and a brief summary of what was said or promised.
I have used this log to catch contradictions that completely changed the trajectory of an appeal. One agent told me the plan required two drug trials before my medication would be covered. A second agent said it only required one. Without a log, that discrepancy disappears. With it, you have evidence of the PBM contradicting its own policy, and that is leverage.
2. Push for a Peer-to-Peer (P2P) Review
Before filing a formal written appeal, ask your doctor to request a peer-to-peer review. This is a phone call between your physician and another medical professional. A five-minute conversation between two doctors can overturn a denial that would have taken weeks of paperwork. Clinical nuances like a specific allergy, a history of adverse reactions, years of successful treatment often land very differently spoken by a doctor than buried in a form.
Be persistent about this. PBMs have been known to "miss" scheduled call windows to avoid the conversation. Have your doctor's office verify that the call was actually scheduled and follow up if it doesn't happen. If an internal appeal has already been denied, your doctor can also use a P2P request to reopen the case for clinical discussion, effectively creating a third opportunity for resolution before escalating to external review.
3. Build a Strong Letter of Medical Necessity
This deserves its own dedicated post, and it has one. But in brief, a Letter of Medical Necessity is not a doctor's note. It is a formal clinical and legal argument that directly addresses the PBM's stated reason for denial, documents your treatment history, cites peer-reviewed evidence, and lays out the clinical consequences of being denied.
For the full breakdown of how to build one that reviewers cannot easily dismiss, see my post on The Ultimate Clinical Argument .
4. Request Your Complete Administrative File
You have a legal right to receive, free of charge, all documents used in making your denial decision. This includes the specific clinical criteria the PBM applied, any internal guidelines or policies referenced, and every piece of information submitted, considered, or generated in the course of the review. Once you have this file, compare it against your actual medical records. PBMs sometimes make their determinations based on incomplete or outdated information. Finding a discrepancy between what they say they reviewed and what your doctor actually documented can be the key that unlocks an appeal.
There is a handy tool called Claim File Helper, by ProPublica that will generate a custom request for you to submit to an insurer to get the notes and documents you are entitled to. Get your claim file before submitting an appeal.
5. Challenge Vague "Medical Necessity" Denials
If your denial says the drug is "not medically necessary," that phrase is not a clinical conclusion, it is a policy position. Demand the specific, evidence-based clinical benchmarks used to reach that determination. What criteria did you fail to meet? What data did the reviewer rely on?
What is your state’s definition of medically necessary? In Tennessee it means
“healthcare services that a physician, exercising prudent clinical judgment, would provide to a patient for the purpose of preventing, evaluating, diagnosing or treating an illness, injury, disease or its symptoms, and that are:
(A) In accordance with generally accepted standards of medical practice;
(B) Clinically appropriate, in terms of type, frequency, extent, site and duration; and considered effective for the patient's illness, injury or disease;
(C) Not primarily for the convenience of the patient, physician, or other healthcare provider; and
(D) Not more costly than an alternative service or sequence of services at least as likely to produce equivalent therapeutic or diagnostic results as to the diagnosis or treatment of that patient's illness, injury or disease;
This matters especially for biologics and specialty medications, where products are often not clinically interchangeable. The FDA's Purple Book lists all licensed biologics and their biosimilars, and it can help your doctor argue why a forced switch to a "similar" medication could be detrimental to a patient who is stable on their current treatment.” Legal definitions hold more water than definitions offered by Pharmacy Benefit Mangers.
6. Verify the Reviewer's Credentials
Most patients never think to do this, and PBMs count on that. Under Tennessee law (TN Code § 56-7-3704(a)(1)), the clinical reviewer who handles your appeal must hold a current medical license and practice in the same specialty area as your prescribing doctor. American Medical Association data shows that only about 16% of insurance "peers" actually have qualifications appropriate to the specific cases they're reviewing.
If you can obtain the reviewer's name and National Provider Identifier (NPI), look them up on the NPI Registry (https://npiregistry.cms.hhs.gov/search). The NPI results should show the provider’s medical license number, which you can then verify is active using your state’s department of health website (https://internet.health.tn.gov/Licensure/). If a generalist or a pediatrician is reviewing a complex adult specialty medication decision, the review may be clinically invalid. Demand a specialist in the same field. Documenting this in your appeal adds significant pressure.
7. Bust the Circular Denial
A circular denial happens when the PBM tells you the claim was denied based on internal criteria, then tells you those criteria are "proprietary" and unavailable to you. This is a stall tactic. Federal laws and regulations such as Employee Retirement Income Security Act (ERISA), Affordable Care Act (ACA, and HIPAA Privacy Rule (45 CFR § 164.524) as well as state PBM reform laws legally entitle you to the clinical rationale and evidence-based references used in your denial. Most denial letters even include a sentence stating you may request these materials free of charge. Do not accept "we can't share that." Put your request in writing and reference the specific legal statute. When the PBM knows you know your rights, the dynamic shifts.
8. Invoke the Expedited 72-Hour Window
For critical or life-sustaining medications, ensure your appeal is submitted as URGENT or STAT. This is not just a label, it triggers a legal requirement for the PBM to issue a decision within 72 hours. Document every stall beyond that window. If they miss the deadline, note it explicitly in any regulatory complaint you file. With one recent appeal, I included a timeline of stall tactics by my PBM along with the growing days of missed treatments and cited the medical harm those missed treatments were causing.
9. Leverage State Regulatory Bodies
If you hit a wall, don't just keep calling the PBM's customer service line. Contact your state's Department of Insurance. In Tennessee, the Tennessee Department of Commerce and Insurance (TDCI) oversees insurance companies and PBMs and can often intervene in ways that individual patients cannot. Filing a formal complaint, especially one that cites specific state codes, signals that you understand the regulatory framework and are prepared to use it.
The NCPA website (https://ncpa.org/pbm-complaints) can help you locate your state's Department of Insurance and access the relevant complaint form, regardless of where you live.
10. Don't Trust Automated Updates
Portal statuses, automated texts, and phone messages are frequently out of sync with each other and with what is actually happening in your file. I have personally received a denial and an approval within the same afternoon, multiple times. Always verify any final decision with a live representative and request the official written determination letter.
Take screenshots of any portal communication indicating approval. Digital portals can be updated or cleared without notice. Physical copies of every letter and every call log are your permanent record and your ammunition for every subsequent round of appeal.
11. Escalate to External Review
If your internal appeals are exhausted, you have the right to an external review handled by an Independent Review Organization (IRO), a third party with no affiliation to your insurance company. Their decision is legally binding on the insurer.
Tennessee residents have an additional protection here. Under TN Code § 56-61-116, the insurer must submit all of your medical records to the IRO within 6 business days. If they miss that deadline, the IRO has the authority to immediately reverse the denial in your favor. You also have 6 business days after your request is accepted to submit additional supporting information. Use that window to include your communication logs, evidence of procedural errors, and any peer-reviewed literature your doctor recommends.
Standard external reviews take approximately 45 days, but urgent cases must be decided within 72 hours. If the IRO reverses the decision, the insurer is legally required to approve coverage immediately.
The Mindset That Makes This Work
Every one of these strategies rests on the same foundation: documentation, persistence, and the willingness to make the PBM work harder to deny you than to approve you. The healthcare system is designed on the assumption that most people will accept the first no and walk away. These power moves exist to prove that assumption wrong.
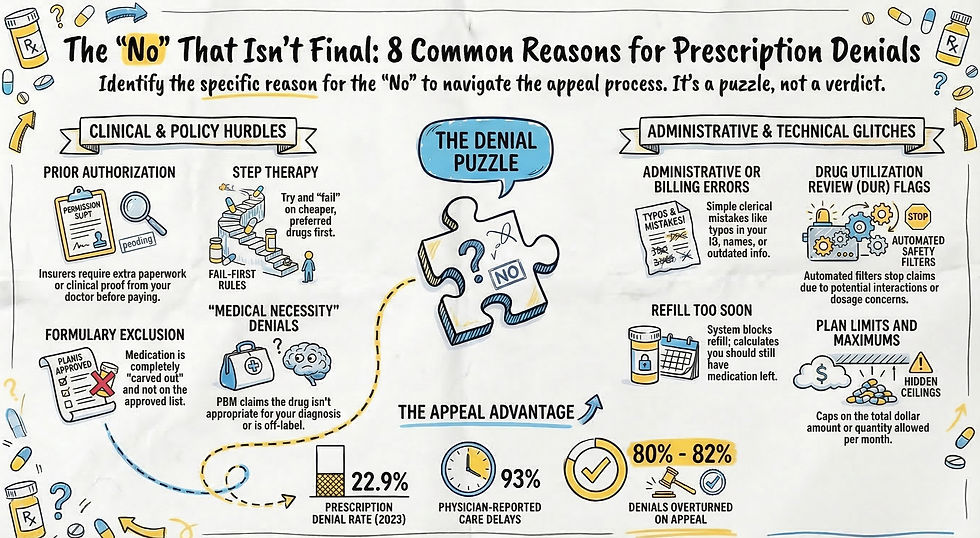
Over 80% of prior authorization appeals are ultimately successful. A denial is not a final verdict. It is an opening offer.
If you want to see how these strategies play out in the real world, including what it looks like when they actually work, read The Ongoing Battle: My Personal Fight Against the PBM Machine.


Comments