
The Ultimate Clinical Argument: Mastering the Letter of Medical Necessity
- Mar 16
- 5 min read
After more than a decade of fighting for my own prescriptions, I can tell you this: the single most powerful document you can put in front of an insurance reviewer is a Letter of Medical Necessity written the right way. Not a rushed paragraph from a rushed doctor. A precise, evidence-backed, legally-aware argument that makes it very difficult for a PBM to say no and even harder to make the denial stick on appeal.
Most patients, and honestly, many providers think a Letter of Medical Necessity (LOMN) is just a doctor's note with a fancy name. It isn't. It is a formal clinical and legal argument, and if you treat it like one, your odds of approval improve dramatically.
Why the Letter Matters More Than You Think
When a PBM denies your prescription, they are making a claim: that your treatment does not meet their definition of "medically necessary." The LOMN is your formal rebuttal. It speaks the reviewer's language — clinical criteria, diagnosis codes, treatment history, supporting literature — and it directly dismantles their stated reason for saying no.
The key word there is "stated reason." Your denial letter must include the specific reason for the denial. If you haven't read yours carefully, go back and find that language. Everything in the LOMN should be aimed at that specific target.
A strong LOMN doesn't just say "my patient needs this." It says "here is the clinical evidence, here is the treatment history, here is what happens if you deny this, and here is why your stated reason does not hold up."

The Five Components of a Winning Letter
1. Administrative and Patient Identifiers
This sounds basic, but missing or incorrect administrative details are one of the most common reasons a letter gets delayed or ignored. The letter must include the patient's full name, date of birth, insurance ID and group number, the claim or case number being appealed, the date of service, and the provider's name, credentials, contact information, and National Provider Identifier (NPI). The NPI is important, it confirms the provider is licensed and qualified. Don't skip it.
2. A Detailed Clinical History
The reviewer needs to understand who this patient is and what their medical journey has looked like. This section should include the specific diagnosis and how long the patient has been under care, a summary of current symptoms and clinical status, and a comprehensive history of prior treatments, what was tried, for how long, and what happened. If previous treatments failed or caused adverse reactions, say so explicitly, with dates and clinical specifics.
If you have been stable on your current medication for months or years, that stability is clinically significant and should be stated clearly. PBMs often process renewals as if you are a brand-new patient, a phenomenon I call "bureaucratic amnesia." Your LOMN can counter that directly by framing the request as a continuation of successful therapy, not a new experiment.
3. Evidence-Based Rationale
This is the heart of the letter, and where most LOMNs fall short. General statements like "this medication is medically necessary" carry almost no weight. What reviewers respond to is specific, documented, evidence-backed reasoning.
Your doctor should directly address the PBM's stated denial reason point by point. If they denied based on step therapy requirements (requiring you to try cheaper drugs first), the letter must explain why those alternatives are clinically inappropriate for this specific patient, whether because they were already tried and failed, because they are contraindicated, or because the patient's condition makes them unlikely to be effective.
Here is a tactic I learned after years of fighting these battles. The prescribing information for your medication, that long document with tiny print sometimes called a "white paper,” is a goldmine of FDA-approved clinical evidence. Your doctor can cite it directly. Peer-reviewed research from sources like PubMed or the Journal of the American Medical Association (JAMA) also carries significant weight. If a study demonstrates that your medication outperforms the PBM's preferred alternative for your specific condition, attach it.
Note for Tennessee residents: Under TN Code § 56-7-3705, your doctor can bypass step therapy requirements entirely if they document that the required alternative is expected to be ineffective or harmful based on your specific medical history. This is a powerful protection. Make sure your LOMN invokes it explicitly if it applies to your situation. If you live outside Tennessee, check your state's insurance laws; many states have similar step therapy override protections.
4. The Consequences of Denial
Do not assume the reviewer understands what happens to a patient who is denied. Spell it out in clinical terms. What is the risk of hospitalization? Is there risk of irreversible harm? Could the patient's condition deteriorate to a point that requires far more expensive interventions? This section should also address the medical necessity standards the treatment meets. Does it prevent the onset of additional illness, reduce the physical effects of the condition, or allow the patient to maintain functional capacity for daily life?
For reauthorization requests, emphasize the patient's positive response to treatment. Stability on a medication is a clinical outcome worth documenting, and it directly argues against "non-medical switching" — being moved to a cheaper alternative not because your health changed, but because the PBM's cost calculations did.
5. Closing, Peer Review Request, and Supporting Documents
The letter should close by requesting a peer-to-peer (P2P) review , a direct conversation between your doctor and a qualified medical reviewer. This is one of the most effective tools available, and a well-written LOMN sets the stage for it.
Include a list of attached supporting documents: chart notes, lab results, imaging reports, and the prescribing information for your medication. The more complete your record, the harder it is for a reviewer to claim they lacked sufficient information.
If your situation is urgent or life-threatening, mark the letter clearly: URGENT: EXPEDITED REVIEW REQUESTED. This is not just a courtesy, it triggers a legal 72-hour decision window that the PBM is required to honor.
A Note on the "Circular Denial"
Watch out for a tactic I have encountered personally, the circular denial. This is when an insurer tells you the claim was denied based on an internal document, then tells you that document is "proprietary" and they cannot share it. Under TN Code § 56-61-107 (and many equivalent state laws), you have a legal right to receive, free of charge, every document relied upon in making your denial decision. If they used it to say no, you are entitled to see it. Don't accept "we can't share that" as an answer.
The Bottom Line
A Letter of Medical Necessity is not a formality. It is your opening argument in what may become a multi-round negotiation. When it is thorough, specific, and evidence-backed, it signals to the PBM that you are not going away and that approving you now is easier than defending a denial later.
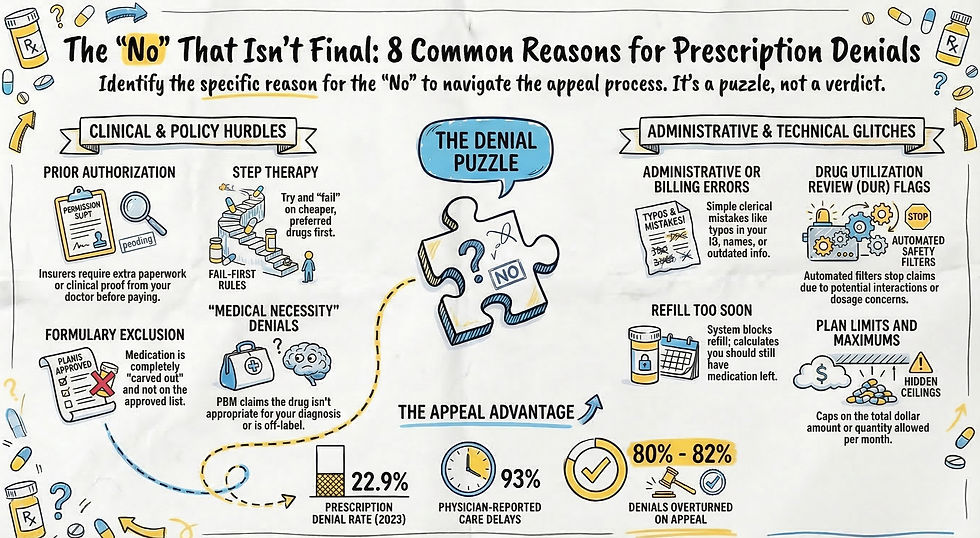
If you want to understand the specific denial reasons your letter needs to address, read my breakdown of The “No” That Isn’t Final: Why Prescriptions Are Denied. And when you are ready to go beyond the letter and deploy the full legal and tactical playbook, explore Beyond the Rejection: Power Moves for Overcoming Denials .


Comments